Day 1 :

Biography:
Guy Hugues Fontaine has made 15 original contributions at the inception of cardiac pacemakers in the mid-60s. He has identified ARVD by serendipity in the late 70s, published 900 scientific papers including 201 book chapters. He is in the 3 books: 216 Profiles in Cardiology since the 14th century (Hurst 2003), “500 greatest Geniuses of the 21th century” (ABI) 2005 USA, the “100 Life time of Achievement” (IBC) 2005 Cambridge UK. Reviewer of 17 journals both in clinical and basic science. He has been invited to give 11 master’s lectures of 90 minutes each during three weeks in the top universities of China (2014). He has also served for 5 years as a Member of the Editorial Board of Circulation. He is also working on brain and heart protection in cardiac arrest and stroke by therapeutic hypothermia. He has recently developed new techniques of hypothermia for brain protection in OHCA and Stroke. This technique has been fortuitously used after resuscitation of his wife at home in June 2011 with absolutely no neurologic deficit despite 6 minutes of no flow. He has also invented a high-tech device which can be considered the ultimate in palliative care by preventing unexpectedly awaking after ordinary sleep. This device was mostly designed for major neurologic disorders.
Abstract:
Histologic demonstration of Atrial Dysplasia in ARVD patients
INTRODUCTION:
Arrhythmogenic Right Ventricular Dysplasia (ARVD) is mainly the result of desmosomal mutations. These mutations may affect both ventricles and atria. However, no histologic demonstration of this condition has been published yet.
OBJECTIVE:
To test the possible presence of a structural anomaly of the atrium in three patients who had ARVD ascertained by histologic material.
METHODS:
We included 3 patients who had typical ventricular histologic pattern of ARVD in whom atrial tissue was collected at autopsy. Histologic slides were obtained after current processing protocol with staining by H&E as well as HPS to have a better identification of bordering or embedding fibrosis which is the hallmark of ARVD.
RESULTS:
The three patients had fat and typical embedding fibrosis and adipocytes similar to what was observed on the right ventricular free wall of ARVD patients. However, one patient had a block of hyaline replacement fibrosis which represent the sequel of myocarditis which is a patchy phenomenon. It was therefore necessary to scrutinised the slides which demonstrated several zones of clusters of lymphocytes suggesting the form of chronic-active myocarditis. Therefore, ARVD patients have also atrial dysplasia which is observed clinically in 80% of cases (Camm HR 2013). The presence of lymphocytes suggests an active process which can be the trigger of arrhythmias (Bonny CRP 2010). As the quiescent form of ARVD is found in 3.7% of the general population there is a new mechanism to explain the frequency of lone atrial fibrillation in young adults in the general population.
CONCLUSION:
Histologic material of atrial dysplasia is demonstrated in patients with ascertained ARVD. The presence of hyaline blocks of fibrosis and clusters of lymphocytes is also similar to the right ventricular structure of ARVD patients. This may contribute to the explanation of the frequency of lone atrial fibrillation in young adults in the general population.
- Track 13: Endocrinology Case Reports
Location: Duai, UAE
Session Introduction
Jamal Abdulkarim
Warwick medical school, UK
Title: Pancreatic Variant Anatomy: The ‘V shaped Pancreas’ – a case report

Biography:
Dr. Abdulkarim had completed his postgraduate training in radiology in Leicester training scheme UK where he obtained the FRCR. Currently he is a Consultant Radiologist at George Eliot Hospital and a visiting fellow to Warwick medical school. Dr Abdulkarim’s current research interest is in the field of reduction of intravenous contrast in CT examination and the effects on renal function where he had published several papers.
Abstract:
ABSTRACT:
Recognition of pancreatic anomalies on imaging is essential as they may be of clinical relevance and are potential causes of recurrent pancreatitis or gastric outlet obstruction in patients. (1)
We describe a ‘V shaped pancreas’, a pancreatic anomaly that resembles canine pancreatic anatomy that, to the best of our knowledge, has not previously been described in humans.
We will also review pancreatic embryological development and anatomy, including common variants.
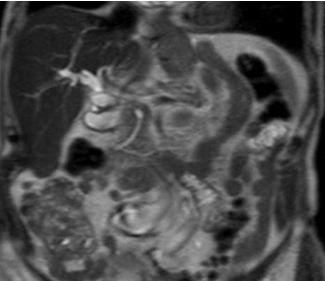
Fig 1: T2 weighted turbo spin echo single shot coronal sequence showing 2 separate moieties of pancreatic tissue separated by fat.
References:
1-Türkvatan A, Erden A, TürkoÄŸlu MA, Yener Ö. Congenital Variants and Anomalies of the Pancreas and Pancreatic Duct: Imaging by Magnetic Resonance Cholangiopancreaticography and Multidetector Computed Tomography. Korean Journal of Radiology 2013;14(6):905-913 doi:10.3348/kjr.2013.14.6.905.
2-Douglas H. Slatter, Textbook of Small Animal Surgery, 2003 - Veterinary surgery
3-Schulte SJ. Embryology, normal variation, and congenital anomalies of the pancreas. In: Stevenson GW, Freeny PC, Margulis AR, Burhenne HJ, editors. Margulis' and Burhenne's alimentary tract radiology. 5th ed. St. Louis: Mosby; 1994. pp. 1039–1051.
4-TaylorAJ, Mortele K. Congenital disorders of the bile and pancreatic ducts [abstr]. In: Abdominal Radiology Course annual meeting program. San Antonio, Tex, 2005; 224–226.
5-Koenraad J. Mortelé, Tatiana C. Rocha, Jonathan L. Streeter, and Andrew J. Taylor. Multimodality Imaging of Pancreatic and Biliary Congenital Anomalies RadioGraphics 2006 26:3 , 715-731
Anas Alghamdi
King Saud Bin Abdul-Aziz University for Health Sciences,Saudi Arabia
Title: Slipped capital femoral epiphysis and primary hyperparathyroidism: A case report

Biography:
Anas A. Alghamdi has completed the Bachelor's of Medicine from college of medicine of King Saud University at Riyadh, Saudi Arabia. Membership of Saudi Diabetes & Endocrine Association. Currently on postgraduation residency training program at King Fahad Medical City.
Abstract:
The aim of reporting this case is to highlight the association of two disorders: primary hyperparathyroidism and slipped capital femoral epiphysis. They are usually seen in two different age groups and rarely together. Primary hyperparathyroidism is a rare cause of slipped capital femoral epiphysis and only ten cases have been reported in the literature worldwide. The patient in our report is a 13-year-old girl who presented to our clinic with bilateral knee pain and a waddling gait. Subsequent investigations showed that she had primary hyperparathyroidism and slipped capital femoral epiphysis with low bone mass. On admission, a parathyroidectomy was performed; then, the slipped femoral epiphyses were fixed with satisfactory results. A systematic algorithmic approach that was illustrated in a previously published case was used. Such cases should be managed in a systematic approach based on the patient’s clinical status to prevent future morbidity. A literature review was conducted by performing a Medline search of all reported cases of primary hyperparathyroidism and slipped capital femoral epiphyses.

Biography:
Dr. Shyam Krishnan has completed his MBBS from B.J Medical College, Pune and Post-graduation in Pulmonary Medicine from Government Medical College, Surat, India.He is currently pursing his fellowship in Interventional Pulmonology at Fortis Hospital, Kolkata, India.
Abstract:
A 44 year old male transferred to our facility from another hospital with a diagnosis of an asthma exacerbation which was not responding to treatment (iv steroids/bronchodilators /antibiotics). He has had 2 admissions in the past 3 months for asthma exacerbations. His complains of shortness of breath on exertion associated with wheezing, nocturnal awakening and dry cough started 6 months ago. Patient denied chest pain, weight loss, fever, chills, night sweats or hemoptysis. No significant past medical history. He was a non-smoker. No history of allergies, nasal discharge, skin disorders. Treatment with bronchodilators did not alleviate symptoms.
On examination the patient was clinically stable. A fixed monophonic wheeze could be heard over the trachea and lung fields. Blood investigations were normal. Pulmonary function studies demonstrated a moderate obstructive pattern with no significant bronchodilator response. Despite a normal chest radiograph the fixed monophonic wheeze on auscultation prompted us to do a CT scan thorax to rule out any endo bronchial pathology. CT Scan demonstrated a polypoid intra-tracheal lesion occupying a 2 cm length of trachea. There was no mediastinal extension or adenopathy. Flexible fiber-optic Bronchoscopy was done which revealed a polypoid intra-tracheal mass occluding approximately 80% of the lumen. The tumor was removed in three sessions by Flexible Bronchoscopy with Argon plasma coagulation and cryosurgery. Histopathological and immunohistochemistry analysis of the resected tumor revealed an intra-tracheal schwannoma. The patient was put on bronchoscopic surveillance for one year with no evidence of recurrence. He is currently asymptomatic.
This case reinforces the common adage that “all that wheezes is not asthma”. Apart from unravelling a rare diagnosis (intra-tracheal schwannoma) the therapeutic role of the bronchoscopic ablative procedures for treatment of intra-tracheal masses are highlighted. More importantly as a result of these advances this patient was spared a major cardiothoracic intervention.
Maswood Ahmad
King Fahad Medical City, Riyadh
Title: An interesting case of neurobrucellosis presenting like pseudotumorcerebri.

Biography:
Dr. Maswood, currently persuing Fellowship in Endocrinology and Metabolism at Obesity, Endocrine and Metabolism Center, King Fahad Medical City, Riyadh. He is M.D. in Internal Medicine from India, actively involved in research recently and have published 5 papers. His feild of interest is Thyroid and General Endocrinology.
Abstract:
Thyrotoxic periodic paralysis (TPP) is a potentially lethal complication of hyperthyroidism characterized by recurrent muscle weakness and hypokalemia. It has been commonly reported in non-Asian populations. Four cases were reported in Saudis so far, and one had a life-threatening arrhythmia. We describe an additional case of a 28-year-old apparently healthy Saudi male patient, who presented with acute paraparesis associated with hypokalemia (K: 2.0 mmol/L), complicated by ventricular tachycardia and cardiac arrest. He was successfully resuscitated and his hypokalemia was corrected. A diagnosis of Graves’ disease associated with TPP was made. He was initially treated with carbimazole and β-blockers and then given a definitive therapy with radioactive iodine, which showed a good response. This case highlights the importance of early recognition and prompt treatment of TPP as a differential diagnosis for muscle weakness. A brief review of TPP and associated arrhythmia is included.
Nawaf Alhazmi
College of Medicine, University of Hail, Saudi Arabia
Title: Relationship between glycated hemoglobin and macrominerals in renal dialysis patients of Hail, Saudi Arabia

Biography:
Nawaf Oudah M Alhazmi is a medical student at College of Medicine, University of Hail, Hail, Kingdom of Saudi Arabia.
Abstract:
Essential minerals have significant role in the glucose metabolism and energy production inside the cell. Imperfect minerals metabolism have been associated with the increased mortality of renal dialysis patients, but their effects in these patients are less characterized. The literature suggested that the incidence of renal dialysis patients in Saudi Arabia showed rapid increase over the last 3 decades. In the present study, we examined the correlations between levels of minerals (serum calcium, phosphorus and magnesium) and HbA1c in diabetic and non-diabetic renal dialysis patients of Hail region. Total 76 blood samples of renal dialysis patients (diabetic and non-diabetic) were analyzed by using biochemical methods. As expected, no significant relationship was observed (p>0.05) in baseline parameters such as age, sodium, potassium, bilirubin, creatinine, urea and glucose, in both diabetic and non-diabetic renal dialysis patients. The results also showed that there is no significant relationship between calcium and phosphorus, calcium and magnesium as well as magnesium and phosphorus in non-diabetic renal dialysis patients; however, in diabetic patients calcium and phosphorus have minor significant association (p=0.057). Further, there was no significant relationship between phosphorus and HbA1c in both types of renal dialysis patients. However, in diabetic renal dialysis patients there was significant relationship (p<0.05) between calcium and HbA1c as well as magnesium and HbA1c. These preliminary results indicate the supportive role of calcium, magnesium and Hb1Ac in the better management of diabetes. The supplementation of calcium and magnesium might be beneficial to manage energy level associated with weakness in the diabetic patients.
- Track 3:Case Reports on Obstetrics & Gynecology
Session Introduction
Badreldeen Ahmed
Feto maternal medicine Centre, Qatar
Title: A case of massive fetal neck tumor

Biography:
Professor Badreldeen is the Director of the Feto-Maternal Medicine Centre in Doha and Professor of Obstetrics at Weill Cornell Medical College – Qatar. He previously held the position of Chairman of Obstetrics and Gynecology at Women’s Hospital, part of Hamad Medical Corporation. Professor Badreldeen was also a consultant obstetrician and gynecologist at Dorset County hospital in Dorchester, UK. His main interests are fetal medicine and high risk pregnancy. Professor Badreldeen is the founding member of the international society of Ultrasound in Obstetrics and Gynecology (ISUOG), a board member of the World Association of Prenatal Medicine, founder and president of the African Association of Perinatal Medicine, founder of the fellowship program in advanced training in obstetrics and gynecology, board member of the Fetus as the Patient Society, founding member of the Academy of Medical Educators and the Regional Director of the Ian Donald School of Medical Ultrasound. Professor Badreldeen has also published over 50 papers in peer-reviewed journals and is the Editor of the ‘Basic book of Ultrasound in Obstetrics and Gynecology’. He has written many chapters in several books, acts as a reviewer for many international journals.
Abstract:
Patient name: R. M,Age: 24
Parity: Para 4 SNVD. Presentation: At 28 weeks of gestation with a neck mass, no other obvious
Anomaly, no polyhydramnios
The mass in the fetal neck is partially solid partially cystic and minimal vascularity, diagnosis of fetal neck teratom was made with US and supported by Antenatal MRI.
Patient was booked for Ex Uterine Intrapartum Treatment (Exit procedure). This procedure will
Offers the advantage of insuring uteroplacental gas exchange While on Placental support.
This is complicated procedure require sophisticated synchronized team work involving multiple disciplines which include:
Fetal medicine specialist, pediatric surgeon, pediatric ENT and neonatologists.
The case management involves different specialties for a better outcome.

Biography:
Dr. Spandan Chaudhary is team leader of Medical Genetics, Diagnostics and Next Generation research divisions of Xcelris Labs, India. He has six years of professional experience in genomics industry specifically in the medical genetics segment. He has developed more than 30 very important diagnostic, sports and nutrition health related assays. He has designed the beta thalassemia mutation screening assay based on whole gene sequencing of HBB gene including all the mutations and indels. He has screened more than 200 individual samples and 25 trio samples as prenatal screening for beta thalassemia. This approach is very useful in diagnosing prenatal thalassemia in combination with regular screening methods
Abstract:
β-Thalassemia is a genetic disease characterized by reduced or non-functionality of β-globin gene expression, which is caused due to number of genetic variations and indels (insertions and deletions). In the present case study, we have reported a rare occurrence of compound heterozygosity of two different variants, namely, HBBc.92G>C and HBBc.92+5G>C in maternal amniotic fluid sample. Prenatal β-thalassemia mutation was detected using nucleotide sequencing method. After analysis, the father was found to be heterozygous for HBBc.92G>C (Codon 30 (G>C)) mutation (β0 type) and the mother was heterozygous for HBBc.92+5GNC (IVS I-5 (G>C)) mutation (β+ type). When amniotic fluid sample was analyzed for β- globin gene (HBB), we found the occurrence of heterozygous allelic pattern for aforesaid mutations. This compound heterozygous state of fetus sample was considered as β+/β0 category of β thalassemia which was clinically and genotypically interpreted as β-thalassemia major. The probability of occurrence of both mutations is very low, because mutations are only 5 base pairs apart on HBB gene. Segregation of compound heterozygosity has occurred twice in this family. Along with the present case, we will share our experience of analyzing 21 unrelated families (trios samples) for detection of β-thalassemia using whole gene sequencing and RT-PCR assays. We will share few interesting case studies like co-inheritance of sickle cell anemia and β-thalassemia traits, compound heterozygosity of beta thalassemia major and normal in the case of twin pregnancy. Prenatal diagnosis helps the parents to know the thalassemic status of the fetus in the first trimester screening.
Snigdha Rao
Institute of medical research, Chandigarh, India
Title: Recurrent fetal hydrocephalus: two rare cases of non-familial hydrocephalus recurring in consecutive pregnancies

Biography:
Snigdha Rao is a final year post-graduate student of the prestigious Post-Graduate Institute of Medical Research, Chandigarh, India. She was the best out-going student of her batch in her MBBS from the prestigious Osmania Medical College, Hyderabad. She was the Joint Secretary of OSMECON-12, Undergraduate National Conference and the Editor-in-chief of the conference magazine. She is interested in pursuing fetal medicine.
Abstract:
Hydrocephalus is one of the most common major congenital anomalies occurring in approximately 0.3 to 1/1000 live births. The etiologies of congenital hydrocephalus include infections, vascular abnormalities, mechanical obstruction and chromosomal abnormalities. In genetic terms, the isolated (non-syndromic) form of hydrocephalus is a primary and major phenotype caused by a specific faulty gene. It is estimated that about 40% of hydrocephalus cases have a possible genetic etiology. It can be X-linked or autosomal recessive or even autosomal dominant. The recurrence risk excluding X-linked hydrocephalus is low. Empiric risk rates range from <1% to 4%. Here we present two cases of non-consanguineous couples with no previous family history presenting to us with fetal hydrocephalus in consecutive pregnancies associated with aqueductal stenosis. In our first case the mother had one neonatal loss due to hydrocephalus, termination of second pregnancy due to same defect and a third live birth with the same defect. In our second case the mother had one neonatal loss due to hydrocephalus, termination of second pregnancy for the same and she came to us for pre-conceptional counseling. Genetic analysis was not done in either case. The correct molecular diagnosis can provide the parents with the recurrence risk together with the possibility of prenatal genetic diagnosis for a future pregnancy.

Biography:
Dr. Abdulkarim had completed his postgraduate training in radiology in Leicester training scheme UK where he obtained the FRCR. Currently he is a Consultant Radiologist at George Eliot Hospital and a visiting fellow to Warwick medical school. Dr Abdulkarim’s current research interest is in the field of reduction of intravenous contrast in CT examination and the effects on renal function where he had published several papers.
Abstract:
Polyorchidism is a rare congenital anomaly described as the presence of more than two testes. The aetiology of this condition is unknown but it was first described by Blasius in 1670 as an incidental finding during an autopsy. This is an uncommon condition particularly with an undescended testis and usually diagnosed at early life. We present a case report of 81 year old with undescended supernumerary testis and to our knowledge this is the oldest age at presentation. We will also discuss the relevant embryological development.

Fig 1: coronal reformat CT image of the abdomen depicting the undescended third testis (seen inferomedial to the left kidney).
References:
- Amodio, John B., et al. "Polyorchidism report of 3 cases and review of the literature." Journal of ultrasound in medicine 23.7 (2004): 951-957.
- Artul, Suheil, and George Habib. "Polyorchidism: two case reports and a review of the literature." Journal of medical case reports 8.1 (2014): 464.
- Avargues, Ana, et al. "Polyorchidism: the case in a young male and review of the literature." Asian journal of andrology 17.3 (2015): 511.
- Bozgeyik, Zülkif, Ercan Kocakoç, and T. Oztürk. "Polyorchidism with lobulation and septa in supernumerary testis." Diagn Interv Radiol 14.2 (2008): 100-2.
- Deveci, Serkan, et al. "Bilateral double testis: Evaluation by magnetic resonance imaging." International journal of urology 11.9 (2004): 813-815.